





Abstract
Continuous positive airway pressure (CPAP) therapy may decrease left ventricular (LV) loads and improve myocardial oxygenation. In this study, we investigated the effect of CPAP on LV diastolic function compared with sham treatment in patients with severe obstructive sleep apnoea (OSA).
This 3-month prospective single-centre randomised sham-controlled trial analysed 52 patients with severe OSA. Patients were randomly assigned (1:1) to receive either CPAP or sham treatment for 3 months. The main investigator and patients were masked to the trial randomisation. The primary end-point was change of early diastolic mitral annular (e′) velocity over the 3-month period. Secondary end-points were pulse wave velocity (PWV), 24-h ambulatory blood pressure (BP) and variables of ventricular-vascular coupling at 3 months.
After 3 months of follow-up, CPAP treatment significantly increased the e′ velocity, and was greater than the sham treatment (0.65±1.70 versus −0.61±1.85 cm·s−1, p=0.014). The PWV, 24-h mean diastolic BP, night-time diastolic BP, arterial elastance index and ventricular-vascular coupling index after 3 months of follow-up decreased significantly in the CPAP group.
In patients with severe OSA, CPAP treatment for 3 months improved LV diastolic function more than sham treatment, and was accompanied by improvements in arterial stiffness and ventricular-vascular coupling.
Abstract
CPAP treatment for 3 months improved LV diastolic function more than sham treatment in patients with severe OSA http://ow.ly/kiYR30ggX5D
Introduction
Obstructive sleep apnoea (OSA) is a common chronic sleep disorder that is characterised by periodic reduction or cessation of breathing due to narrowing of the upper airways during sleep [1]. OSA is thought to be related to heart failure [2–4], as well as hypertension [5, 6], myocardial infarction [7] and arrhythmia [8], and exhibits episodic hypoxaemia, nocturnal sympathetic nervous system activation, elevated blood pressure (BP), and markers of oxidative stress, inflammation and hypercoagulability [9, 10].
Left ventricular (LV) diastolic dysfunction is often observed in patients with OSA, and is accompanied by common comorbidities, such as hypertension, obesity and diabetes, and consequent arterial stiffness and LV hypertrophy [11–14]. OSA contributes to the development of LV diastolic dysfunction and subsequent heart failure, even in patients with preserved ejection fraction [3, 4, 11]. Recent studies have suggested partial reversal of LV diastolic dysfunction after continuous positive airway pressure (CPAP) therapy through improved myocardial oxygenation, diminished LV pressure overload and sympathetic activation [13, 15, 16]. However, there were limited data proving the benefits of CPAP therapy on LV diastolic function from a randomised, sham-controlled clinical trial.
Therefore, in this study, we hypothesised that CPAP therapy for 3 months in patients with severe OSA would improve LV diastolic function when compared with sham treatment. In order to prove our hypothesis, we measured the effects of CPAP therapy on LV diastolic function in patients with severe OSA using comprehensive echocardiographic evaluations before and after 3 months of therapy. Moreover, we sought to characterise the underlying mechanisms involving LV diastolic dysfunction by a comprehensive assessment of arterial stiffness, BP variables and ventricular-vascular coupling.
Methods
Study design and patients
A prospective, single-centre, randomised, sham-controlled trial of parallel groups was conducted at Severance Hospital (Seoul, Republic of Korea). The trial was designed to determine the 3-month effects of CPAP on LV diastolic function in patients with severe OSA. This study was approved by the Severance Hospital institutional review board and registered with www.clinicaltrials.gov (NCT01854398). All patients provided informed consent.
60 patients with a confirmed diagnosis of severe OSA were enrolled. Severe OSA was defined as an apnoea/hypopnoea index (AHI) >30 events·h−1, as established by overnight polysomnography using the recommended hypopnoea criteria of the American Academy of Sleep Medicine (AASM) [17]. All participants were screened according to their history, clinical examination, baseline blood tests, 12-lead ECG and transthoracic echocardiography results. Exclusion criteria were LV ejection fraction <50%, prior history of coronary artery disease, arrhythmia, significant valvular dysfunction (of a moderate or greater degree), uncontrolled BP (≥180/110 mmHg), chronic kidney disease (estimated glomerular filtration rate <60 mL·min−1) or treatment with anxiolytics or sedatives. 56 eligible consenting patients underwent baseline BP measurements (peripheral BP, central BP and 24-h ambulatory BP monitoring), pulse wave velocity (PWV) determination and diastolic stress echocardiography.
Randomisation and masking
After baseline evaluation, patients who met eligibility criteria were randomly assigned (1:1) into parallel groups to receive either CPAP therapy (n=28) or sham therapy (n=28) for 3 months. Random assignment of patients was based on computer-generated random numbers unknown to the investigators. All patients were masked to the treatment. Thus, they were not aware whether they were receiving CPAP treatment or sham treatment. The investigators who assessed the end-points were unaware of the randomisation status of the patients, and did not set up or maintain the machines or assist the patients. The neurologist (Yang-Je Cho) who was assigned to monitor the treatment did not participate in end-point assessments. Therefore, despite the physical nature of the treatment, the study was effectively double blind.
Procedures
Patients were provided with a CPAP machine (S9 Elite with H5i; ResMed, San Diego, CA, USA). All study patients underwent standard CPAP titration to deliver pressures of 4–20 cmH2O to eliminate obstructive events. CPAP titration was performed at the hospital as manual titration under full polysomnography, and patients received fixed pressures. Patients who were randomised to the sham interventions were fitted with one of two nasal mask interfaces (Mirage FX Nasal Mask or Swift FX Nasal Pillows Mask; ResMed) and scheduled for a full night of polysomnography using sham-CPAP. The sham system had modified masks which had an internal flow restricter and additional holes for effective washout of carbon dioxide. The sham system was designed to provide a patient experience similar to the true CPAP therapy. The pump-tubing-mask system with exhalation ports of sham equipment delivered similar sensations of flow from the mask and provided visual user interface feedback and operating sounds; however, the sham system was designed to deliver subtherapeutic CPAP of <1 cmH2O.
Patients in the CPAP group started fixed-pressure CPAP at titrated pressure. Over a 3-month period, patients visited the neurologist on a monthly basis, and CPAP pressure was adjusted according to the results generated by the CPAP machine. CPAP compliance was monitored and/or recorded at patients’ monthly visits throughout the study. CPAP was considered to be satisfactory when used minimally for 4 h per night for ≥6 nights per week. 26 OSA patients completed this part of the study with a mean duration of CPAP therapy of 3 months before the second examination.
During the 3 months, two patients in each group discontinued interventions. All measurements were repeated after the 3-month study period. Ultimately, 52 patients were analysed for the end-points (figure 1). We checked that any drugs taken for hypertension had not been changed.

Trial profile. BP: blood pressure; CPAP: continuous positive airway pressure.
Polysomnography
Overnight polysomnography was performed using Embletta X100 system (Natus Embla Systems, Oakville, ON, Canada), a type-2 fully unattended portable system approved by the AASM. This type-2 portable monitor incorporates a minimum of seven channels, including two electroencephalography channels. This allowed accurate calculation of the AHI and was an improvement over the rough estimates that were obtained by type-3 or -4 portable systems [18]. Manual laboratory CPAP titration was performed using in-laboratory polysomnography (REMStar Auto; Respironics, Pittsburgh, PA, USA and Comet XL system; Grass Technologies, West Warwick, RI, USA).
Diastolic stress echocardiography
Diastolic stress echocardiography with simultaneous respiratory gas analysis was performed using a variable load bicycle ergometer (Medical Positioning, Kansas City, MO, USA) with the subject in the supine position. Echocardiographic examination was performed simultaneously using ultrasound machines (Vivid 7 or Vivid E9 system; GE Healthcare, Chicago, IL, USA) with a 2.5-MHz transducer as described previously [19, 20]. From the resting images, standard two-dimensional and Doppler measurements were performed per the recommendations of the American Society of Echocardiography [21]. From the apical windows, a 1–2-mm pulse Doppler sample volume was placed at the mitral valve tip. The mitral inflow velocities were traced, and the following variables were obtained: peak velocity of early (E) and late (A) filling, and deceleration time of the E wave velocity. Stroke volume was measured from the LV outflow track diameter and pulse wave Doppler results. Early diastolic (e′) and systolic (s′) velocities of the mitral annulus were also measured on an apical four-chamber view with a 2–5-mm sample volume placed at the septal corner of the mitral annulus.
After obtaining standard rest images, multistage supine bicycle exercise testing was performed using a variable-load bicycle ergometer. The subjects pedalled at a constant speed beginning at a workload of 25 W, with an incremental workload of 25 W every 3 min until limited by their symptoms. All measurements were performed at rest and at each stage of exercise in the same sequence. All data were digitally stored and analysed by two experienced sonographers who were blinded to the clinical and central haemodynamic data.
End-systolic pressure (ESP) was estimated as systolic BP×0.9, as described previously [22]. Arterial elastance (Ea) was estimated as ESP/stroke volume. The arterial elastance index (EaI) was estimated by normalising the Ea to body surface area [23]. End-systolic ventricular elastance (Ees) was calculated by ESP/end-systolic volume [23]. Then, the ventricular elastance index (EesI) was calculated by normalising the Ees to body surface area. Finally, the ventricular-vascular coupling index was determined by the EaI/EesI ratio. These measurements were performed at baseline, 25 W and 50 W of exercise in the same sequence.
Arterial tonometry
The radial pulse wave and PWV were assessed by arterial tonometry (SphygmoCor; AtCor Medical, Sydney, Australia). These measurements were collected in the supine position after a minimum rest of 5 min just before echocardiography. Central systolic BP, diastolic BP, pulse pressure (PP), augmentation pressure, augmentation indices, an index normalised for a heart rate of 75 bpm (AIx@75) were derived using pulse waveform analysis techniques. PP amplification was calculated as the ratio of peripheral to central PP. PWV was assessed at rest using the quotient of the carotid-femoral path length and carotid-femoral pressure pulse transit time. Pressure waveforms were gated with simultaneous electrocardiography and were used to calculate the PWV between two sites. Tonometry transit distances from the suprasternal notch to the radial, femoral and carotid recording sites were measured using a tape measure. The distances between recording sites were adjusted for parallel transmission in the aorta and the carotid sites by correcting for the distance between the suprasternal notch and the carotid site.
The 24-h ambulatory BP monitoring
Ambulatory BP monitoring was performed using an appropriately sized BP cuff on the nondominant arm, using a BP monitor (model 90207; SpaceLabs, Snoqualmie, WA, USA) programmed to record the BP every 30 min throughout the 24-h period. Mean 24-h BP was calculated as the mean of all the readings throughout the 24-h period. Night-time BP was defined as the BPs from the time the patient went to bed until the time the patient got out of bed, and daytime BP was defined as the BPs recorded during the rest of the day. Patients with ±10% change in night-time BP from daytime BP were considered to be nondippers.
Outcomes
The primary end-point was the change of early diastolic mitral annular (e′) velocity over the 3-month trial period. Secondary end-points were PWV, 24-h ambulatory BPs and variables of ventricular-vascular coupling at 3 months. In addition, we performed a subgroup analysis of treatment effects in patients according to the presence or absence of hypertension, baseline LV diastolic function and the severity of OSA (AHI <50 events·h−1 or ≥50 events·h−1). Baseline diastolic function was classified into either preserved or impaired myocardial relaxation according to age-stratified normal reference of e′ velocity: e′ <10 cm·s−1 in patients aged ≤40 years and e′ <7 cm·s−1 in patients aged >40 years were considered to represent impaired myocardial relaxation [24].
Statistical analysis
We chose a target sample of 60 patients to achieve >46 patients reaching the 3-month assessment of the primary end-point. We calculated this sample size to provide 90% power with an α-value of 0.05. We expected a reduction of 20% in participants resulting from dropout because of withdrawals during the 3 months. A statistical analysis plan was completed before undertaking any data analyses. Group allocation was masked during the analysis of the primary outcome. The primary and secondary end-points were analysed in the per-protocol population.
Continuous variables are presented as mean±sd and categorical variables as a percentage of the group total. Differences between the two groups were analysed using two-sample t-tests. Paired comparisons before versus after CPAP or sham treatment were performed using paired t-tests. A p-value <0.05 was considered statistically significant. All analyses were performed in SPSS (version 22.0; IBM, Armonk, NY, USA).
Results
Baseline characteristics
Between May 1, 2013, and June 30, 2016, we recruited and screened patients for eligibility. 60 patients were eligible and we randomly assigned 28 to the sham treatment and 28 to the CPAP treatment. The per-protocol population was 26 patients in the sham therapy group and 26 patients in the CPAP therapy group. Their baseline characteristics are shown in table 1. There were no differences between the two study groups, with the exception of higher body mass index and a higher prevalence of dyslipidaemia and statin usage in the CPAP group. The proportions of subject with hypertension in both groups were not different and the medication histories for BP control were comparable. Baseline polysomnography characteristics were not statistically different between the two groups.
Baseline characteristics of the study population
Adherence to the intervention
Mean duration of use of the CPAP device did not differ between the two groups (4.6±1.2 h·day−1 for the active CPAP group and 5.0±1.6 h·day−1 for the sham group, corresponding to 450 accumulated CPAP hours over 3 months for the CPAP group, and 414 accumulated CPAP hours over 3 months for the sham group). In the active CPAP group, the residual AHI during the 3 months of the trial intervention, measured by CPAP devices, averaged 3.5 events·h−1, indicating good control of OSA with active CPAP.
Effects on LV diastolic function
The effects of CPAP and sham treatment on LV structural or functional parameters are shown in table 2. LV structural variables including LV dimension, LV mass index and relative wall thickness were comparable between the two groups and were not changed significantly after the study period. LV ejection fraction and s′ velocities, which were markers of LV systolic function, were in the normal ranges in both groups either at baseline or after follow-up. In terms of LV diastolic function, the baseline e′ velocity in the CPAP group (7.7±2.2 cm·s−1) was significantly lower than that in the sham group (9.4±2.7 cm·s−1; p=0.017), suggesting a more impaired LV relaxation in the CPAP group. Similarly, baseline E/e′, reflecting LV filling pressure, was significantly higher in the CPAP group than in the sham group. However, after the 3-month treatment, those values were similar in both groups. The 3-month CPAP treatment revealed a significant improvement of LV diastolic function compared with the sham treatment (change of e′ velocity 0.65±1.70 versus −0.61±1.85 cm·s−1; p=0.014) (figure 2a).
Echocardiographic variables at baseline and 3 months after treatment

Changes of myocardial relaxation and arterial stiffness in the two study groups. a) Early diastolic mitral annular tissue (e′) velocity; b) pulse wave velocity (PWV). CPAP: continuous positive airway pressure. *: p<0.05 by t-test, compared with the corresponding sham group.
Effects on BP and arterial stiffness
As shown in table 3, peripheral BPs, central BPs and PP amplification in the two groups were not different at baseline and follow-up. Moreover, the changes of each parameter after 3 months of treatment were not significant in both groups. The PWV in the CPAP group at follow-up decreased considerably (7.2±1.0 m·s−1) compared to either baseline values (8.0±1.3 m·s−1; p<0.001) or the corresponding values (8.1±1.0 m·s−1; p=0.004) in the sham-treated group (figure 2b). Therefore, the change of PWV during the 3-month treatment was significantly different between the groups (−0.05±1.11 m·s−1 in the sham group versus −0.80±1.08 m·s−1 in the CPAP group; p=0.023).
Peripheral, central and 24-h ambulatory blood pressure (BP) variables at baseline and 3 months after treatment
In terms of 24-h ambulatory BPs, night-time diastolic BPs and mean diastolic BPs at the 3-month follow-up in the CPAP group were significantly lower than the baseline values before randomisation. However, these BP-lowering effects were not visible in the sham-treated group.
Effects on ventricular-vascular coupling
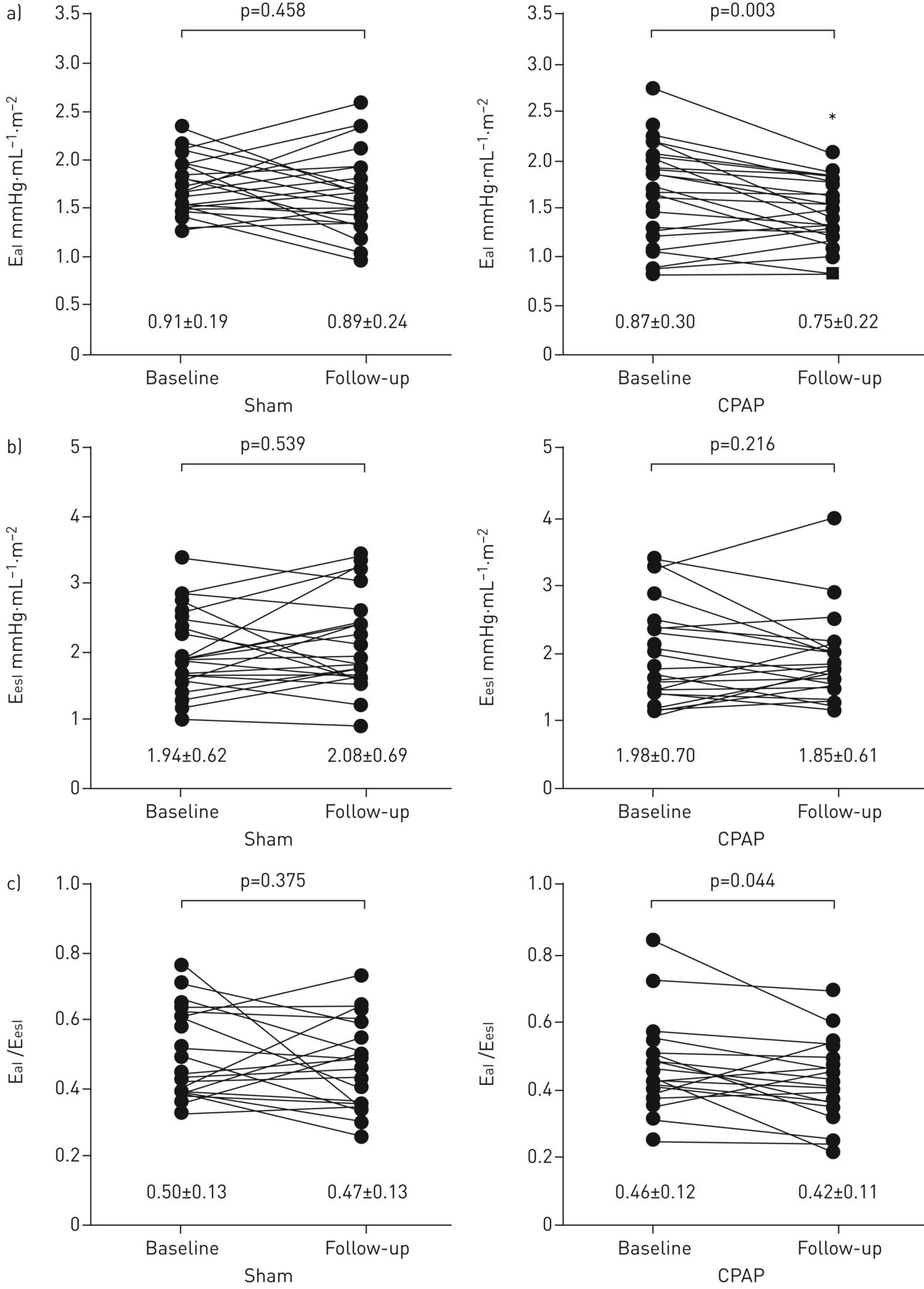
Table 4 and figure 3 display each component of ventricular-vascular coupling and their changes in both groups. Baseline values of end-systolic volume index, stroke volume index, ESP, EaI, EesI and EaI/EesI were similar in both groups. However, resting stroke volume index at the 3-month follow-up in the CPAP group (40.1±7.7 mL·m−2) was significantly higher compared with the corresponding value in the sham group (35.7±5.7 mL·m−2; p=0.026). In the CPAP group, EaI at rest and at 25 W and 50 W exercise decreased significantly after the 3-month treatment. Finally, the ventricular-vascular coupling index (EaI/EesI) at rest decreased considerably in the CPAP group (p=0.044), but not in the sham group (p=0.375).
Ventricular-vascular coupling at baseline and 12 weeks after randomisation
{kind=link}
{kind=link}
{kind=link}
Changes of a) arterial elastance index (EaI), b) ventricular elastance index (EesI) and c) ventricular–vascular coupling index (EaI/EesI) in the two study groups. CPAP: continuous positive airway pressure. *: p<0.05 by t-test, compared with the corresponding sham group.
Changes of LV diastolic function and arterial stiffness in the subgroups
Table 5 shows the results from subgroup analyses according to the presence of hypertension, baseline LV diastolic function and the severity of OSA. The results suggest that patients with hypertension and less severe OSA (30≤AHI<50 events·h−1) would be more likely to benefit from CPAP therapy in improved LV diastolic function and arterial stiffness. Patients with both preserved and impaired myocardial relaxation showed significant benefits from CPAP therapy, compared to those in the sham group.
Subgroup analyses according to baseline characteristics
Discussion
The results of this trial indicate that 1) treatment with CPAP for 3 months in patients with severe OSA resulted in significantly improved LV diastolic function compared to sham treatment; 2) treatment with CPAP for 3 months in patients with severe OSA resulted in a significant improvement of arterial stiffness compared to sham treatment; and 3) significant enhancement of ventricular-vascular coupling was observed in the CPAP group and this result was associated with improved arterial elastance. To the best of our knowledge, the present study is the first to comprehensively demonstrate the effects of CPAP on LV diastolic function and the pathophysiological mechanisms in patients with severe OSA, using a randomised, sham-controlled clinical trial.
Observational studies have suggested that OSA contributes to the development of LV diastolic dysfunction and subsequent heart failure, even in patients with preserved ejection fraction [3, 4, 11]. Although several studies have suggested a role for OSA as an independent risk factor for the development of diastolic dysfunction, there have been inconsistent data, depending on the methodological approaches used to detect early diastolic dysfunction and the selection of the study populations [13, 25, 26]. In a study by Kim et al. [26], only patients with severe OSA showed a significant impairment of LV diastolic function as assessed by e′ velocity from tissue Doppler imaging, and LV diastolic dysfunction was associated with the severity of OSA independent of body mass index, diabetes mellitus and hypertension. Therefore, in the present study, we evaluated LV diastolic function using diastolic stress echocardiography as well as tissue Doppler imaging to detect early diastolic dysfunction and its changes after CPAP treatment in patients with severe OSA.
CPAP is the standard therapy for patients with OSA. Recent studies have shown a partial reversal of LV diastolic dysfunction after CPAP therapy through improved myocardial oxygenation, diminished LV pressure overload and sympathetic activation [13, 15, 16]. A previous prospective randomised placebo-controlled crossover study reported that chronic application of nasal CPAP avoided the progression of diastolic abnormalities and might reverse these alterations, at least in the initial stages before the development of severe structural changes [13]. However, LV diastolic function was assessed by conventional Doppler parameters, such as the E/A ratio, deceleration time and isovolumic relaxation time, which are currently considered less sensitive and indirect measures of LV diastolic function than the e′ velocity obtained from tissue Doppler imaging. Therefore, in the present study, we evaluated LV diastolic function based on current clinical practice and guidelines, including tissue Doppler imaging techniques. Furthermore, changes in ventricular-vascular coupling were assessed from haemodynamic and volumetric assessment of the LV and systemic artery, because arterial stiffness and the resulting LV systolic and diastolic stiffness have been highlighted as key contributors to the pathophysiology of heart failure with preserved ejection fraction [27–29]. In addition, we have provided results regarding the improvement of LV diastolic function after CPAP treatment in comparison to sham treatment and have proposed a pathophysiological link between LV diastolic function and arterial stiffness through an improved LV diastolic function along with improved arterial stiffness, decreased night-time diastolic BP and decreased resting and exercise arterial elastance.
Previous studies reported that CPAP therapy promotes significant BP reduction [30, 31]. In the current study, we found no significant improvement of peripheral BPs, central BPs and PP amplification. However, it should be noted that patients with uncontrolled BP were excluded from this study. In addition, almost half of the patients did not have hypertension, and the rest had already well-controlled hypertension at baseline. Such baseline characteristics may have precluded significant reduction of peripheral and central BPs. Interestingly, CPAP therapy significantly improved night-time diastolic BP and PWV compared to those in the sham group. We believe that effective CPAP therapy contributes to an increase in oxygenation and a reduction of sympathetic activity, as well as improvement of night-time BP.
Also of interest in this study was a significant increase in stroke volume after CPAP treatment compared with sham treatment, and this could be related to the pathophysiological effects of OSA on LV preload and afterload described in previous studies [2, 32, 33]. The combination of increased LV afterload, by surges in sympathetic nervous system activity and BP, and diminished LV preload, by leftward displacement of the interventricular septum at the time of exaggerated negative intrathoracic pressure against the occluded upper airway, have been reported to cause progressive reductions in stroke volume and cardiac output [2, 32, 33]. Moreover, it has been shown that treatment of OSA via CPAP largely reversed the overnight decreases in stroke volume and cardiac output [33], although the study was not a randomised, sham-controlled study. Likewise, one study demonstrated that CPAP treatment for 26 weeks in moderate to severe OSA with hypertension significantly improved ventricular-vascular coupling via a significant reduction in EaI [34]. However, the present study is the first to show the beneficial haemodynamic effects of CPAP therapy in severe OSA, compared with sham treatment, by a prospective, randomised clinical trial. A recent randomised trial without a sham control suggested that CPAP did not improve diastolic dysfunction in patients with coronary artery disease [35]. In our study, we excluded patients with coronary artery disease to avoid confounding comorbidities that affect diastolic function other than OSA. Additional sham-controlled randomised trials are needed to determine whether the benefit of CPAP therapy expands to OSA patients who are at high risk of cardiovascular problems.
The results from subgroup analyses provided important insights concerning the optimal therapeutic timing of CPAP in severe OSA regarding the aspects of reversing LV diastolic dysfunction. Despite the small number of patients, patients with AHI <50 events·h−1 showed a significant improvement of e′ velocity in the CPAP group compared with the sham group, but patients with AHI ≥50 events·h−1 did not. These findings suggested that reversal of LV diastolic function after 3 months of CPAP therapy can be achieved if the severity of OSA is not extreme. In addition, patients with hypertension tended to experience more benefits from CPAP therapy. In summary, the results demonstrated that the pathophysiological mechanism relating to LV diastolic dysfunctions were linked to decreasing arterial stiffness.
Our study has some limitations. First, we excluded patients with reduced LV ejection fraction, a history of coronary artery disease, uncontrolled hypertension, significant valvular dysfunction and/or arrhythmia. Thus, our results should only be applied to populations that are similar to those eligible for our study. Second, despite randomisation, there were some between-group differences in baseline characteristics. The baseline e′ velocity in the CPAP group was lower than that in the sham-treated group. To adjust for the different baseline characteristics, the data were analysed in subgroups according to the baseline characteristics. In addition, regression analysis was performed in order to adjust differences in baseline characteristics; the change of e′ velocity was still significant in the active CPAP group compared to the sham group, even after adjustment of baseline characteristics (online supplementary table S5). Third, we included only two females in each group, so further studies are warranted in order to have confidence in our results for females with severe OSA. Last, some unidentified confounding factors might have affected the LV diastolic function during the 3-month treatment. However, we determined that cardiac medications and body weights did not change during the study period.
In conclusion, CPAP treatment for 3 months improved LV diastolic function more than sham treatment, and was accompanied by improvements in arterial stiffness and ventricular-vascular coupling in patients with severe OSA.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Tables S1–S5 ERJ-01774-2017_supplementary_tables
Acknowledgements
We thank the patients who participated in our trial and their relatives; ResMed for providing research equipment; and all physicians and research staff members for their hard work and enthusiasm.
Author contributions: G-R. Hong and Y-J. Cho designed this study after literature search. C.Y. Shim, S. Park, H-J. Cho and G-R. Hong contributed to the data collection. C.Y. Shim, D. Kim, Y-J. Cho and G-R. Hong contributed to the data analysis and interpretation. C.Y. Shim, D. Kim and C.J. Lee performed the statistical analysis of the primary end-points and reviewed other statistical analyses. C.Y. Shim and D. Kim wrote the first draft of the report. S. Park, H-J. Cho, J-W. Ha, Y-J. Cho and G-R. Hong reviewed and revised the manuscript critically for important intellectual content before submission. All authors approved the final submitted version.
Footnotes
This article has supplementary material available from erj.ersjournals.com
This study is registered at www.clinicaltrials.gov with identifier number NCT01854398.
Support statement: This study was supported by a Yuhan research grant and a faculty research grant at Yonsei University. Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interest: None declared.
- Received August 30, 2017.
- Accepted October 30, 2017.
- Copyright ©ERS 2018
References










