Telehealth Is Here to Stay: Opportunities and Challenges for Cancer Care
In Partnership With:

Oncology practices across the United States have rapidly increased telehealth use in 2020 to mitigate the risk of coronavirus disease 2019 (COVID-19) to patients with cancer who are at particular risk of complications.


Ryan Nguyen, DO

Oncology practices across the United States have rapidly increased telehealth use in 2020 to mitigate the risk of coronavirus disease 2019 (COVID-19) to patients with cancer who are at particular risk of complications. The initial results from the COVID-19 and Cancer Consortium Registry cohort study (NCT04354701) showed a case-fatality rate of 13% (compared with 2.9% among the general population, according to the Johns Hopkins Coronavirus Resource Center1) among patients with a history of cancer and COVID-19, with increased age, increasing comorbidities, worse performance status, and active cancer as independent risk factors for increased mortality.2 Not only do patients with cancer face higher risks of morbidity and mortality if they contract the virus, they also face the challenges that arise with the inevitable delays in anticancer therapy during recovery f rom COVID-19.

Shikha Jain, MD, FACP

At the University of Illinois Cancer Center (UICC), we have seen a marked increase in the use of telehealth services from March 2020 that continues as we enter month 6 of the COVID-19 pandemic. Shifting selected in-person clinic visits to telehealth has helped us both reduce patients’ exposure risks and protect health care providers and patients who require in-person care from additional exposures. As health systems across the nation begin shifting to “business as usual,” many cancer practices and their patients will continue to use telehealth as a risk-reduction tool to augment cancer care. However, careful attention is needed to address barriers to delivering high-quality medical care via telehealth.
Regulator Relief
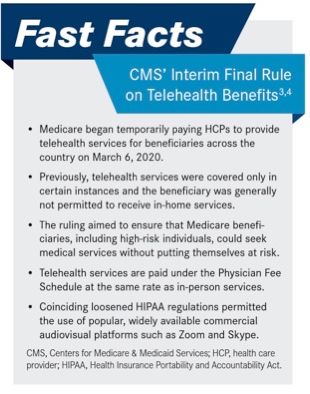
In March 2020, the Centers for Medicare & Medicaid Services (CMS) released an interim final rule that reduced barriers to telehealth access as COVID-19 cases grew in the United States (FAST FACTS3,4).Whereas CMS previously covered telehealth only when a patient was receiving care in a facility in a nonurban area or in an area in a health professional shortage, telehealth could not be delivered directly to a patient’s home prior to the pandemic. CMS also dropped the requirement for telehealth recipients to have a prior relationship with a health care professional, allowing physicians to conduct new patient consultations via telehealth. The loosening of Health Insurance Portability and Accountability Act regulatory requirements on telehealth technologies for providers acting in good faith also allowed physicians and their patients to use widely available commercial audiovisual platforms such as Zoom and Skype. Finally, CMS increased compensation for telehealth visits to match the fee schedule for in-person services.4


Fast facts3,4
Telehealth Boom
The loosening of regulatory requirements led to a boom in telehealth use across health care. Findings of a study of New York University urgent care visits showed a 135% increase in telehealth visits from March 2, 2020, to April 14, 2020.5 According to results of an April 2020 McKinsey & Company consumer survey, consumer adoption of telehealth jumped from 11% in 2019 to 46% in 2020. The burst in telehealth usage also led to an increase in patients who feel comfortable using telehealth, with 76% of survey respondents reporting they were “highly” or “moderately” likely to use telehealth going forward.6
Choosing Visits Appropriate for Telehealth
Successful implementation and integration of telehealth into cancer care requires identifying which in-person services can be rendered safely and effectively with this modality. The American Society of Clinical Oncology special report on cancer care during the COVID-19 pandemic identifies eligible telemedicine visit types: COVID-19–positive infections, nonurgent high-risk patient populations, and symptom management.7 At UICC, to ensure patients scheduled for telehealth visits are appropriate, our team triages clinic schedules 1 week in advance to allow patients time to adjust their schedules and arrange transportation. Although attending physicians determine which visits may be converted to telehealth encounters, patients with more urgent questions or clinical needs are always offered the option of in-person services. Our teams have found telehealth to be an effective means of communicating with patients regarding nonurgent matters, and patients often appreciate not having to commit the time and transportation resources for issues that can be addressed with a phone call.
Challenges in Equitable Telehealth Delivery
COVID-19 has further exposed disparities in access to care for vulnerable populations. Although opportunities exist for telehealth to address and improve upon inequities in the health care system, the rapid shift to telehealth services also has the potential to widen disparities in access to care. Accessibility to a stable phone or broadband connection can be a challenge in rural areas or for patients with limited income. Among Americans older than 65 years, who make up 18% of the American population and are most likely to need chronic disease management, just 55% to 60% own a smartphone or have home broadband access. Low-income individuals have lower rates of smartphone ownership (71%), home broadband access (59%), internet use (82%), and basic digital literacy (53%).8 Also limiting the effectiveness of telehealth is the comfort of both physician and patient with use of telehealth technologies and digital health literacy. In our experience, we have found most patients to be comfortable with telephone-only visits, with a minority comfortable consistently using audiovisual communication. Patient subgroups with known limited digital literacy and access include older adults, low socioeconomic status, limited health literacy, limited English proficiency, and racial and ethnic minorities.
Although many of the conversions from in-person visits to telehealth encounters are well intentioned and provide opportunities for more accessibility for certain populations, for patients with limited access to telehealth, we opt to prioritize a return to in-person visits. As we traverse this pandemic and nimbly adapt and implement effective strategies to provide exceptional patient care to all our patients, it is essential that we assess the risks and benef its of the transition to telehealth visits with the potential barriers and limitations that may unintentionally negatively affect our patients. Every effort should be made to reduce the risk of COVID-19 to our patients, but we must also take into consideration how to best deliver equitable medical care to our at-risk patient populations and whether that can be delivered effectively with telehealth.
References
- Mortality in the most affected countries. Johns Hopkins Coronavirus Resource Center. Accessed September 30, 2020. https://coronavirus.jhu.edu/data/mortality
- Kuderer NM, Choueiri TK, Shah DP, et al; COVID-19 Cancer Consortium. Clinical impact of COVID-19 on patients with cancer (CCC19): a cohort study. Lancet. 2020;395(10241):19071918. doi:10.1016/S0140-6736(20)31187-9
- President Trump expands telehealth benefits for Medicare beneficiaries during COVID-19 outbreak. News release. Centers for Medicare & Medicaid Services. March 17, 2020. Accessed September 30, 2020. https://www.cms.gov/newsroom/ press-releases/president-trump-expands-telehealth-benef its-medicare-beneficiaries-during-covid-19-outbreak
- Royce TJ, Sanoff HK, Rewari A. Telemedicine for cancer care in the time of COVID-19. JAMA Oncol. Published online July 16, 2020. doi:10.1001/jamaoncol.2020.2684
- Mann DM, Chen J, Chunara R, Testa PA, Nov O. COVID-19 transforms health care through telemedicine: evidence from the field. J Am Med Inform Assoc. 2020;27(7):1132-1135. doi:10.1093/jamia/ocaa072
- Bentsennyy O, Gilbert G, Harris A, Rost J. Telehealth: a quarter-trillion-dollar post-COVID-19 reality? McKinsey & Company Healthcare Systems & Services. May 29, 2020. Accessed September 30, 2020. https://www.mckinsey. com/industries/healthcare-systems-and-services/our- insights/telehealth-a-quarter-trillion-dollar-post-covid- 19-reality
- ASCO special report: a guide to cancer care delivery during the COVID-19 pandemic. American Society of Clinical Oncology. May 19, 2020. Accessed September 30, 2020. https://www.asco.org/sites/new-www.asco.org/files/ content-files/2020-ASCO-Guide-Cancer-COVID19.pdf
- Nouri S, Khoong EC, Lyles CR, Karliner L. Addressing equity in telemedicine for chronic disease management during the COVID-19 pandemic. NEJM Catal Innov Care Deliv. Published online May 4, 2020. https://catalyst.nejm.org/ doi/full/10.1056/cat.20.0123