Two cases of circumflex coronary anomaly arising from RCA: one of them with inferior STEMI and VT
#CardioTwitterCase originally published on Twitter
The origin of circumflex from the main RCA has a reported incidence of 0.37 %. Here are two very unusual cases of an anomalous origin of the left circumflex coronary artery from the proximal RCA, one of them with inferior STEMI and VT.
These cases were originally published on Twitter by @JuanGuzmnOlea2
Case 1
Clinical presentation
A 61-year-old male patient referred to the cathlab for right and left cardiac catheterizations due to mitral valve disease with severe stenosis.
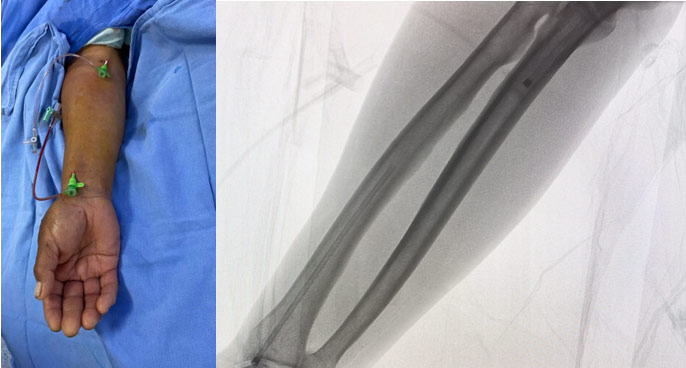
A venous and arterial access through right forearm was performed using basilic vein and proximal radial artery. A 6 French introducer sheath was placed (Figure 1).
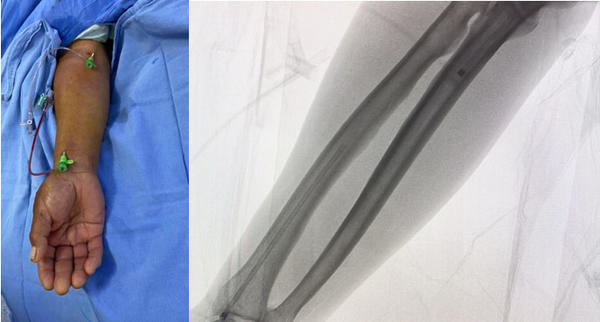
Figure 1.
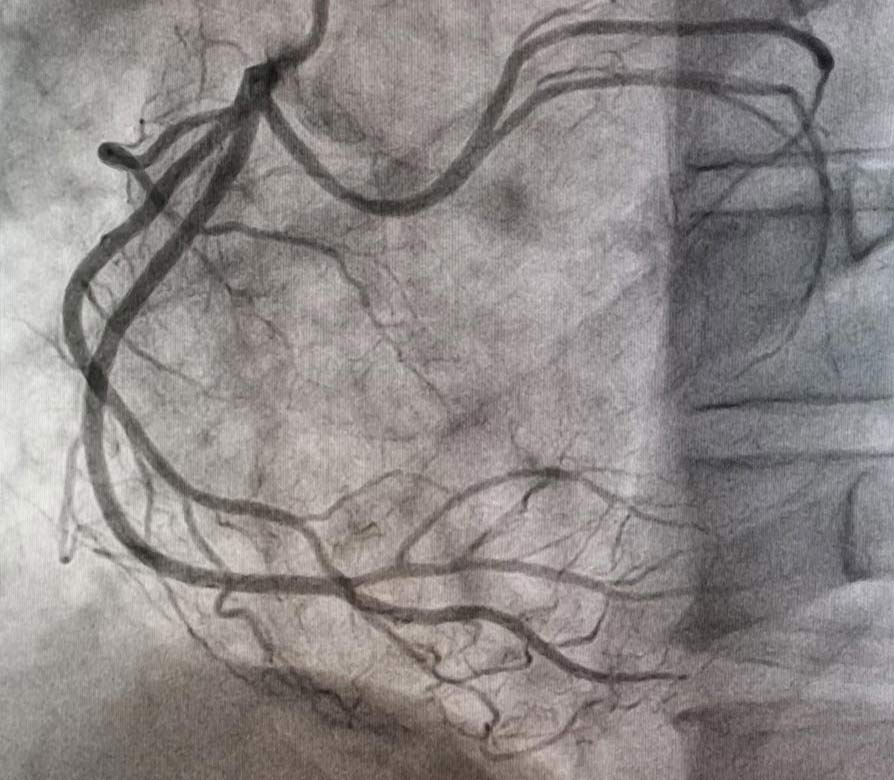
The coronary angiography revealed left system LAD and ramus without lesions, RCA no lesions, and anomalous origin of the circumflex coronary artery from the proximal segment of the RCA without lesions. (Figure 2 and Video 1).
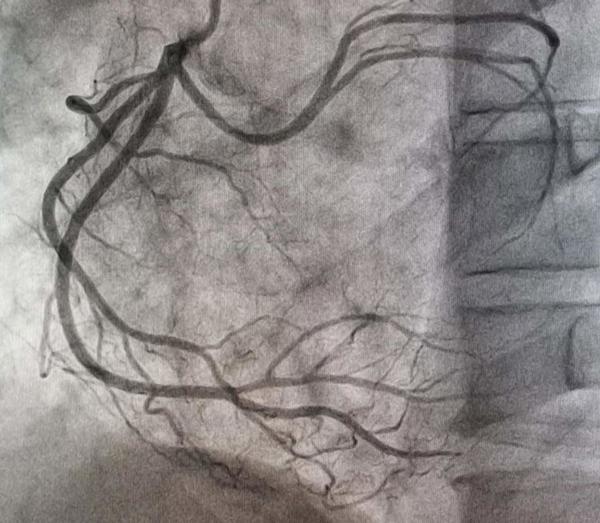
Figure 2.
A severe calcified mitral valve was also documented, together with double lesion with transmitral gradient of 28 mmhg and moderate insufficiency (++/++++ Sellers), LVEF 60 %, in addition to severe pulmonary hypertension.
The case was then to be discussed by the heart team.
Case 2
Clinical presentation
A 57-year-old man with smoking as a modifiable cardiovascular risk factor and no cardiovascular history. He presented oppressive chest pain of more than 20-minute span accompanied by tachycardia and diaphoresis.
He immediately went to the emergency service of the hospital and the initial electrocardiogram revealed ventricular tachycardia that was resolved with electrical cardioversion. The electrocardiogram after cardioversion documented an inferior STEMI (Figure 3).
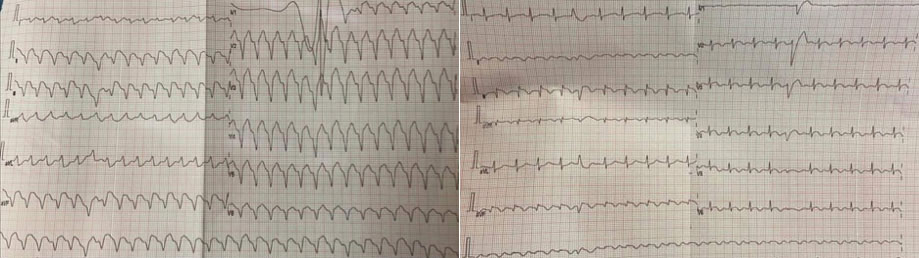
Figure 3.
He was sent to the interventional cardiology department for primary angioplasty. Proximal right radial approach and 6 French introducer sheath were used.
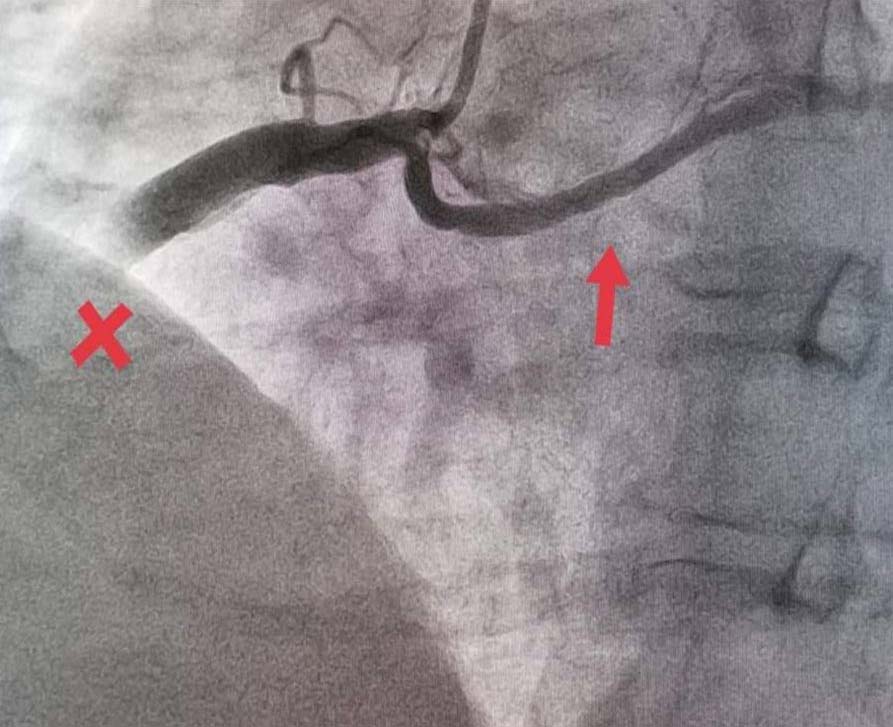
The coronary angiogram revealed left system without lesions, ectatic RCA with acute total occlusion in the middle segment with grade 5 thrombus, and anomalous origin of the circumflex coronary artery arising from the proximal segment of the RCA with fusiform aneurysm in its middle portion (Figure 4 and Figure 5).
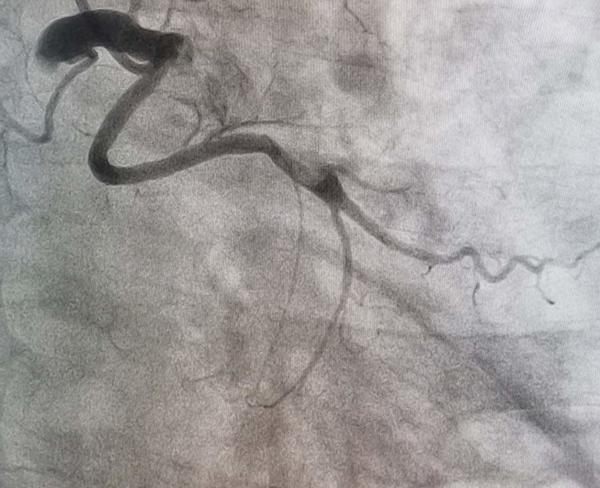
Figure 4.
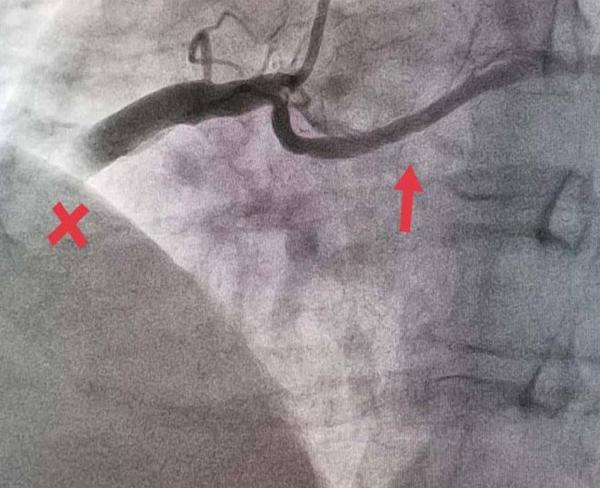
Figure 5.
We proceeded to intervention, used JR4 6Fr guide catheter and advanced distally a 0.014” Runthrough floppy guidewire, then advanced a Pronto V4 thromboaspiration system obtaining large thrombus load, use glycoprotein IIb/IIIa inhibitors.
After that, a 3.0 x 15 mm balloon was advanced to predilate occlusion site, and then 4.0 x 20 mm balloon to posdilate, observing distal flow to posterior descending, however still with a large thrombus load and a very ectatic vessel (Video 2).
We decided to continue with dual antiplatelet therapy and glycoprotein IIb/IIIa inhibitors.
We performed a control angiogram 72 hours later, nevertheless, still with a large thrombus load in a very ectatic vessel, and we decided to continue with oral anticoagulation.
Final remarks
According to some publications, anomalous LCx are divided into 3 types :
- type I: separate ostia for RCA and LCx;
- type II: common ostia in the right sinus;
- type III: LCx arising as a branch of the proximal RCA.
The last type, as presented in these cases, is the least common, with a reported incidence of 0.37 %.
They can be found in stable or unstable settings where, even if the occlusion of the right coronary artery was proximal, it could lead to a more catastrophic scenario.
Original tweet and Twitter discussion
Two cases of circumflex coronary anomaly arising from RCA. One of them with inferior STEMI and VT@BotPci@mirvatalasnag@Ortega_Paz@mmamas1973pic.twitter.com/FfTwATccTy
— Juan Guzmán Olea (@JuanGuzmnOlea2) July 3, 2021
Authors


No comments yet!