





Abstract
The poor representability of real-life patients in severe asthma RCTs is closely related to the selection of end-points. A composite criterion to evaluate the benefit/risk balance rather than separate end-points would broaden the eligible population. http://ow.ly/JLel30naY1Y
To the Editor:
We read with interest the paper by Brown et al. [1], which confirms the lack of external validity in randomised controlled trials (RCTs) of phenotype targeted biological therapies in severe asthma. Our team conducted a very similar study several years ago and we are pleased the present study reaches consistent findings [2]. Of 593 asthmatic patients from the French COBRA cohort, 303 were considered severe asthmatics (Global Initiative for Asthma criteria [3]) and were assessed against eligibility criteria of RCTs targeting severe asthma. The eligibility rates ranged from 0.27% to 10.71%. The data presented by Brown et al. [1] highlight the lack of improvement over the past years. These findings raise major ethical issues in medical decisions, at both the individual and collective levels.
RCT methodology ensures the internal validity of results and is often considered sufficient to label the conclusions as “evidence-based”. However, the lack of external validity compromises the extrapolation of study results. For nine out of 10 patients with severe asthma, the extrapolation of RCTs results is not evidence-based, as per our own conclusions [2] and those of Brown et al. [1]. At the collective level, the implementation of guidelines/health policies based on results with poor external validity to the whole target population is hazardous and counterproductive.
The identification and understanding of the implementation of narrow criteria are crucial. This is the first step in improving external validity for a reliable management of patients and populations.
In pharmaceutical industry-sponsored RCTs, the choice of eligibility criteria is multifactorial. The aim of such trials (especially phase III trials) is to demonstrate that the risk/benefit balance of a drug warrants its market access. For economic and commercial reasons, trials should be performed as quickly as possible. Thus, three main parameters drive the selection of the study population:
1) Demonstrating efficacy and safety is easier when potential responders are recruited and subjects at predictable risk of adverse events are excluded.
2) From a statistical perspective, homogenising a study population decreases the number of subjects needed and/or the duration of the study, which has obvious economic advantages.
3) Market access requires the validation of the results by regulatory agencies through their own efficacy end-points.
Basically, RCTs enrol homogeneous populations of potential responders to the study drug as per regulatory agencies' criteria.
As mentioned by Brown et al. [1], “regulatory authorities have a major influence over the design of RCTs.” In the European Medicines Agency guidelines some efficacy end-points are recommended for the development of asthma medications: “In general, for a new controller treatment the preferred end-point is exacerbation… Lung function should be measured either as a co-primary or a key secondary end-point” [4].
Thus, a patient must have room for improvement in forced expiratory volume in 1 s (FEV1) when entering a clinical trial, which means a persistent airway obstruction with possible reversibility.
Moreover, patients must experience several exacerbations per year to enable the detection of a decreased annual rate without extending the duration of studies beyond 1 year. This may explain why a majority of trials in severe asthma require both persistent airflow obstruction and frequent exacerbations while the concomitant occurrence of these criteria is not required to consider a diagnosis of uncontrolled severe asthma in real life.
Brown et al. [1] divided the eligibility criteria into “diagnostic criteria” and “biomarker criteria” and highlighted the most discriminating criteria are “heterogeneous diagnostic criteria aiming to reconfirm a diagnosis of asthma”. Accordingly, it is surprising that these do not reflect the American Thoracic Society/European Respiratory Society severe asthma criteria [5]. This finding challenges the authors as these criteria exclude a majority of patients while providing only “arbitrary diagnostic labels”. We do not believe these are “diagnostic criteria”. We interpret their implementation as a way to select potential responders to enable the demonstration of efficacy.
Finally, Brown et al. [1] mainly focus on the impact of these inclusion criteria on external validity, but consequences of exclusion criteria should not be neglected. Subjects at risk of adverse events are often excluded from RCTs. This is particularly true for the elderly and patients with multimorbidities, two overlapping subgroups of patients [6]. In our study, we identified 10% of patients excluded from RCTs because of the “age” criterion and an additional 2% because of comorbidities.
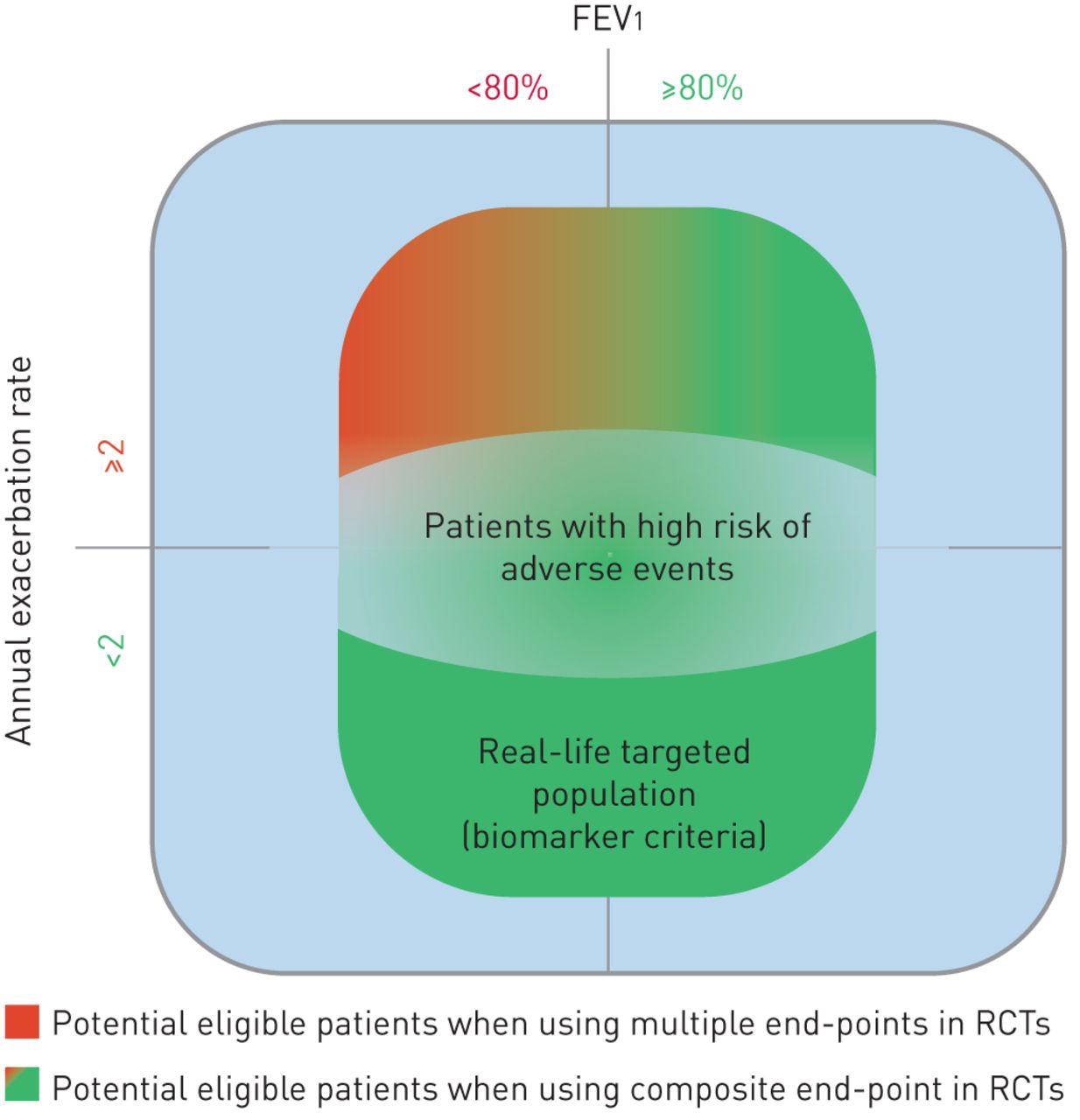
Overall, the lack of external validity due to a poor representability of real-life patients in RCTs targeting severe asthma is closely related to the selection of efficacy and safety end-points. In real-life practice, risk/benefit balance is evaluated through multiple end-points (FEV1, exacerbation rate, quality of life, asthma control, adverse events and their severity). We believe that the use of a composite criterion to evaluate the benefit/risk balance as the primary end-point rather than separate end-points would enable the demonstration of efficacy while broadening the eligible population. Indeed, this would enable the inclusion of different clinical phenotypes, decrease the number of events needed in each category of criteria to observe efficacy and allow the occurrence of adverse events if overweighed by clinical benefit (figure 1).
{kind=link}
The variation in the proportion of severe asthma patients potentially eligible for biotherapy-evaluating randomised controlled trials (RCTs) can be visualised in function of the considered end-point (multiple end-points versus composite end-point). FEV1: forced expiratory volume in 1 s.
Footnotes
Conflict of interest: L. Pahus has nothing to disclose.
Conflict of interest: D. Jaffuel has nothing to disclose.
Conflict of interest: I. Vachier has nothing to disclose.
Conflict of interest: A. Bourdin has been an investigator in clinical trials for and received grants, personal fees and non-financial support from GSK, has been an investigator in clinical trials for and received grants and personal fees from AstraZeneca, Boehringer Ingelheim, Novartis, Chiesi Farma and Teva, has been an investigator in clinical trials for PneumRx, has been an investigator in clinical trials for and received personal fees from Actelion, and received grants from Merck, outside the submitted work.
Conflict of interest: C.M. Suehs has nothing to disclose.
Conflict of interest: N. Molinari has nothing to disclose.
Conflict of interest: P. Chanez reports grants and personal fees for consultancy, advisory board work and lectures from Almirall, Boehringer Ingelheim, Centocor, GSK, AstraZeneca, Novartis, Teva, Chiesi, ALK and Boston Scientific, and grants from AMU, outside the submitted work.
- Received November 16, 2018.
- Accepted November 20, 2018.
- Copyright ©ERS 2019










