Eleven Weeks of Iron Supplementation Does Not Maintain Iron Status for an Entire Competitive Season in Elite Female Volleyball Players: A Follow-Up Study

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and methods
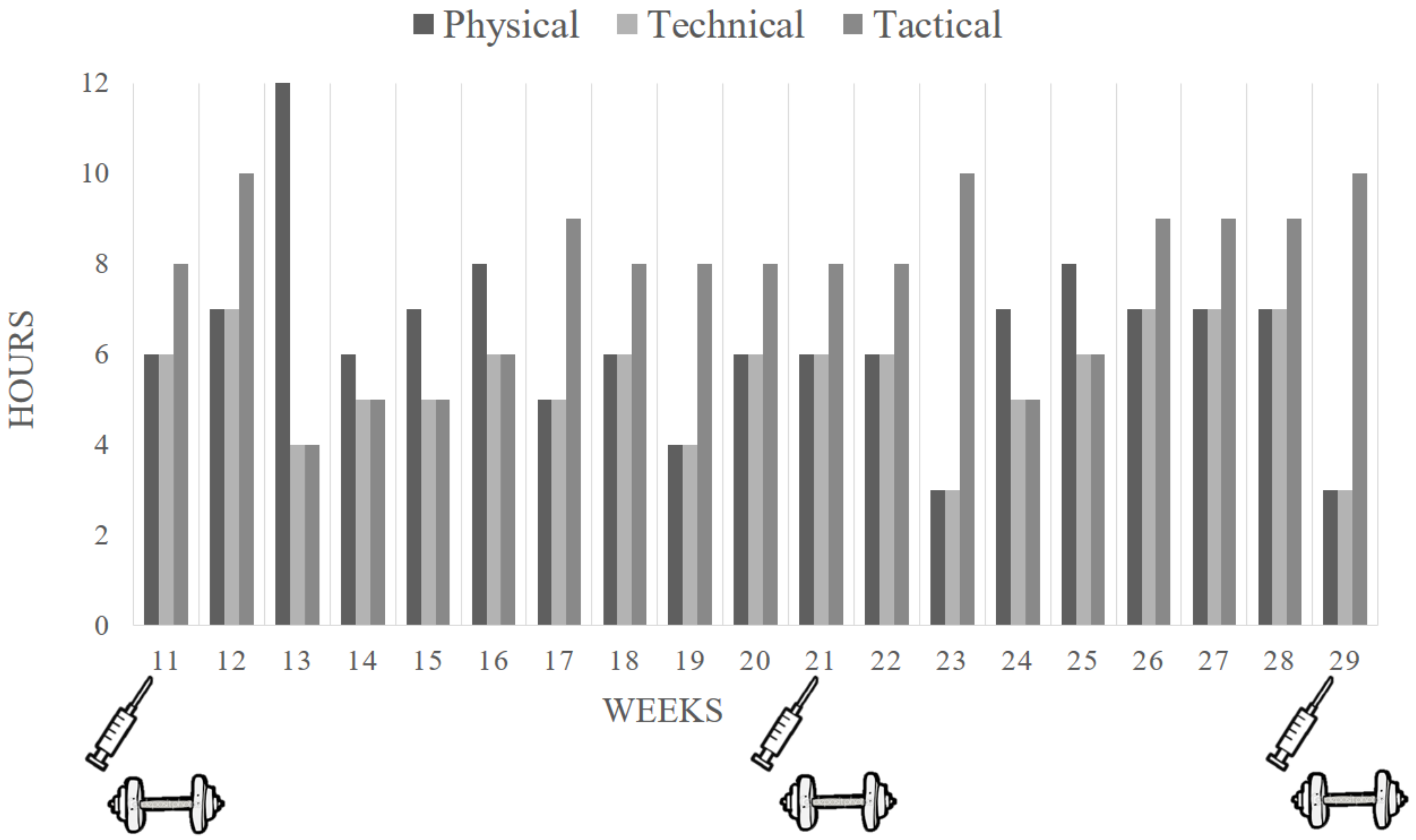
2.1. Brief Description of the Previous Supplementation Period
2.2. Study Design and Participants
2.3. Iron Status Categorization
2.4. Blood Collection and Analysis
2.5. Strength Performance Testing
2.6. Dietary Assessment
2.7. Statistical Analyses
3. Results
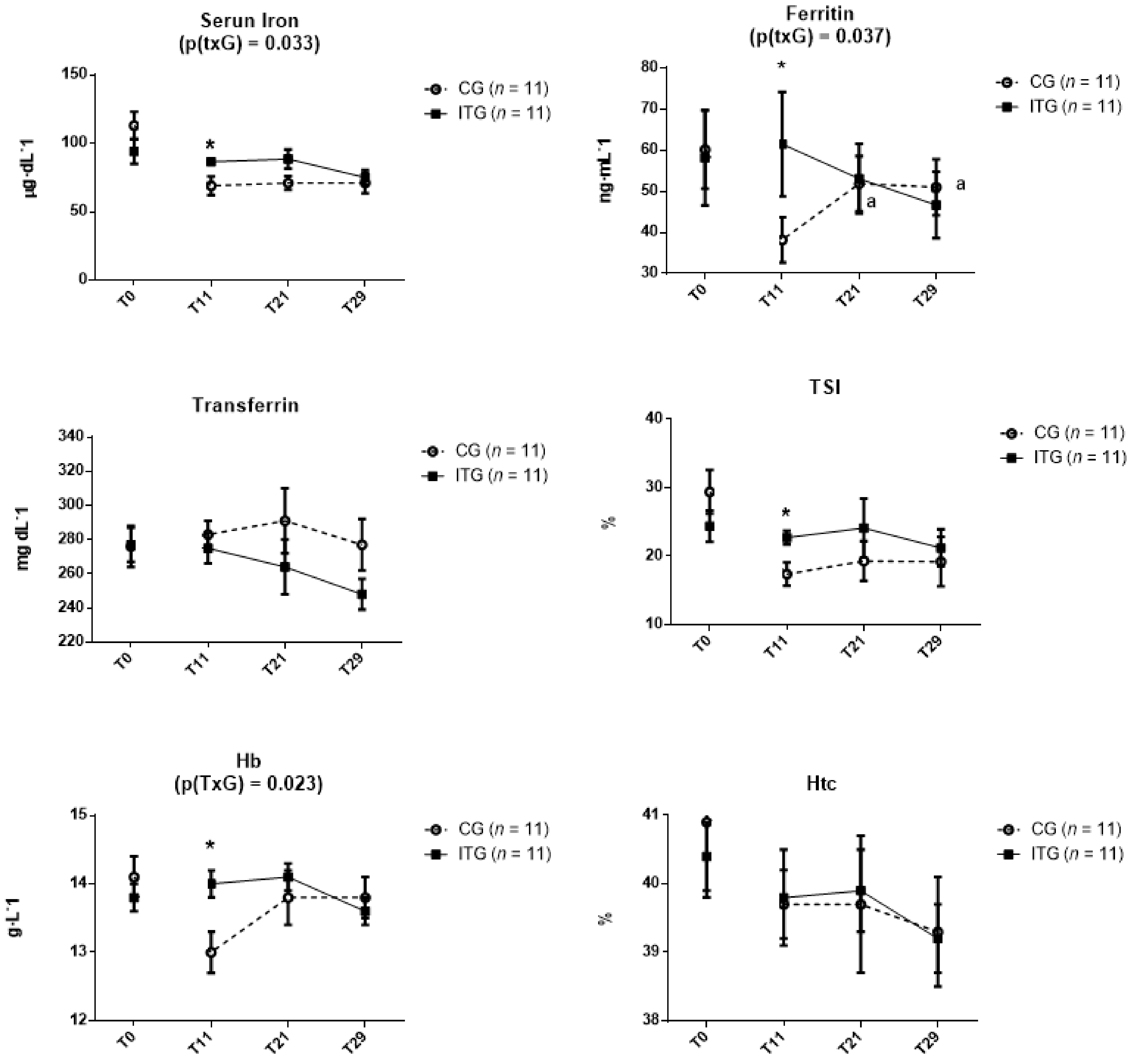
3.1. Haematological Parameters
3.2. Iron Status Categorization
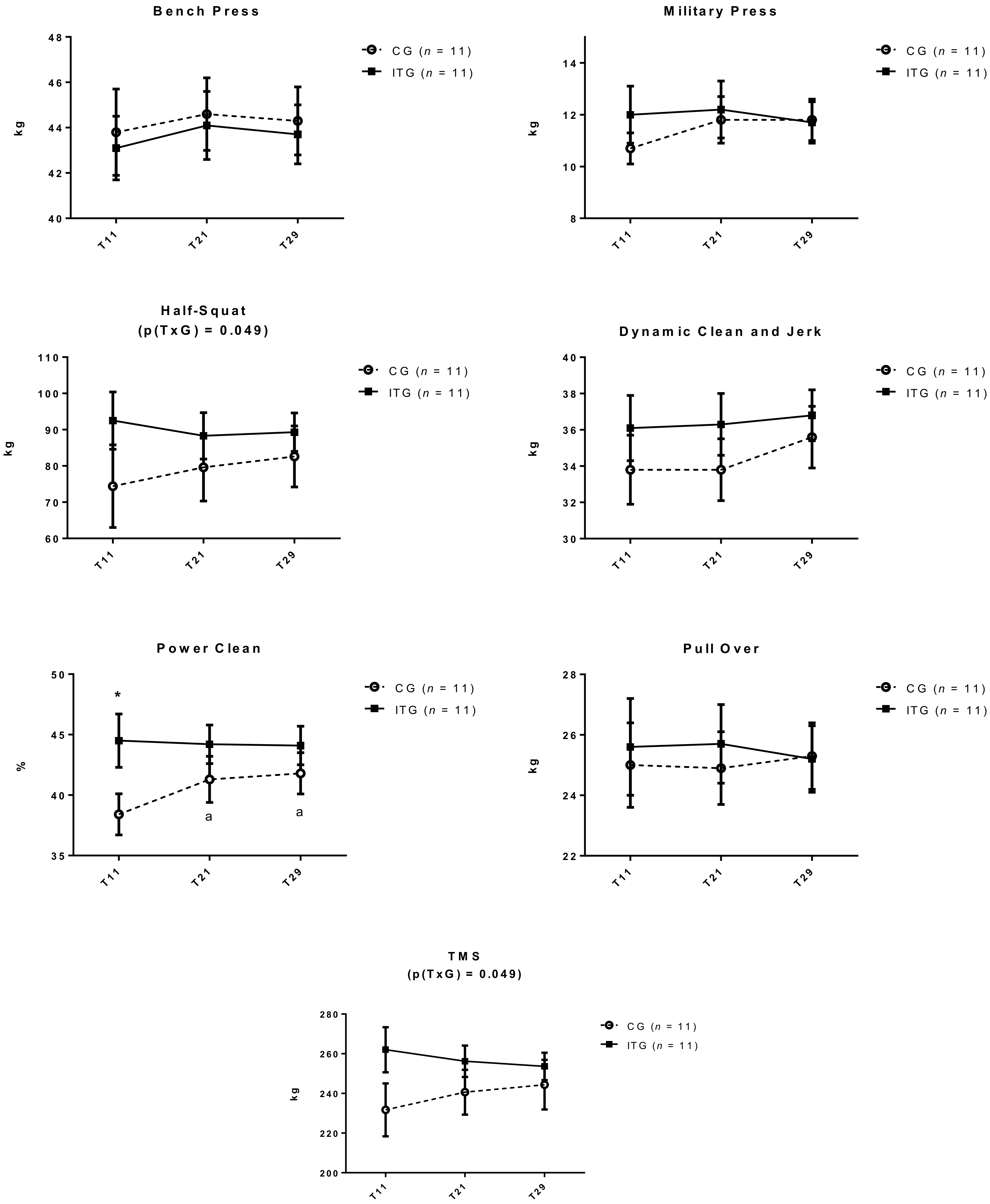
3.3. Strength Performance Tests
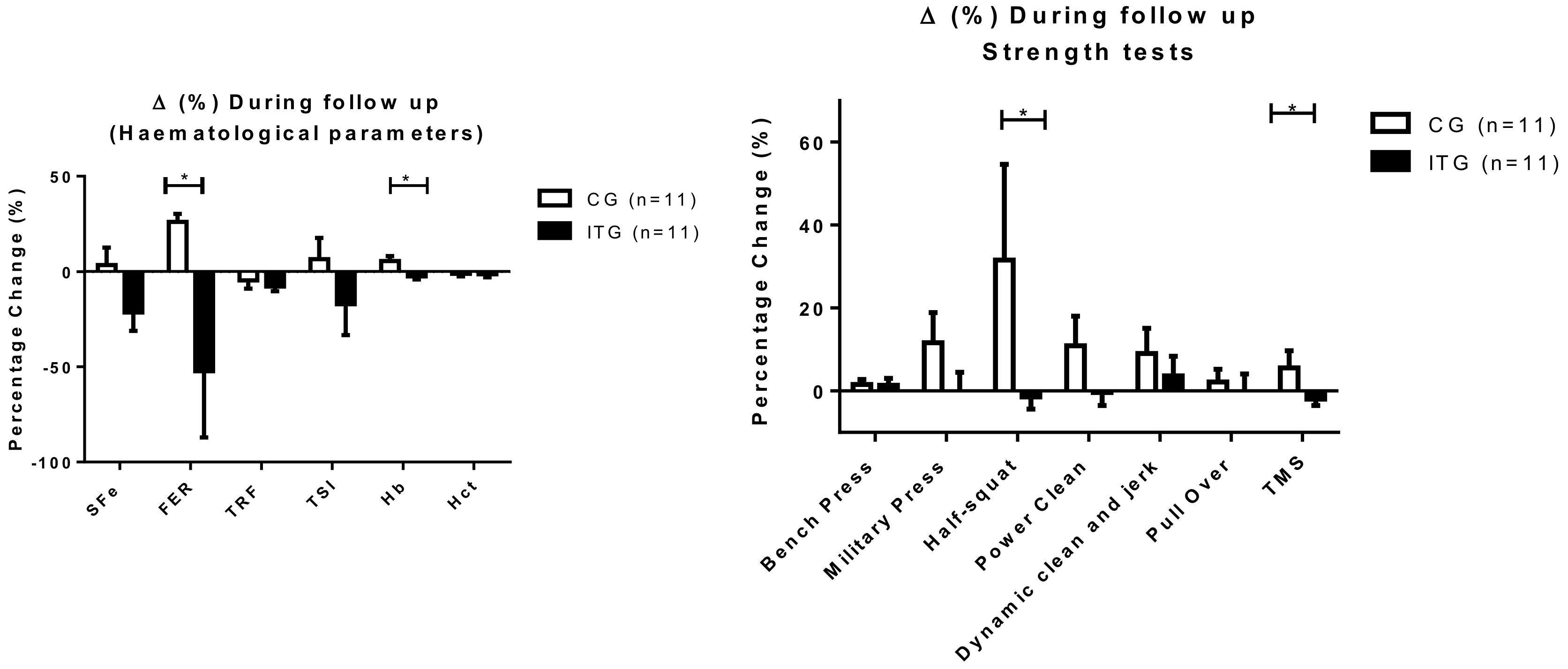
3.4. Percentage Changes Differences for Hematological and Strength Parameters.
3.5. Relationship Between Hematological and Strength Changes
3.6. Dietary Intake
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgements
Conflicts of Interest
References
- Hinton, P.S. Iron and the Endurance Athlete. Appl. Physiol. Nutr. Metab. 2014, 39, 1012–1018. [Google Scholar] [CrossRef] [PubMed]
- Shaskey, D.J.; Green, G.A. Sports Haematology. Sports Med. 2000, 29, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, A.; Enayatizadeh, N.; Akbarzadeh, M.; Asadi, S.; Tabatabaee, S.H. Iron Status in Female Athletes Participating in Team Ball-Sports. Pak. J. Biol. Sci. 2010, 13, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Mielgo-Ayuso, J.; Urdampilleta, A.; Martinez-Sanz, J.M.; Seco, J. Dietary Iron Intake and Deficiency in Elite Women Volleyball Players. Nutr. Hosp. 2012, 27, 1592–1597. [Google Scholar] [PubMed]
- Brownlie, T., 4th; Utermohlen, V.; Hinton, P.S.; Haas, J.D. Tissue Iron Deficiency without Anemia Impairs Adaptation in Endurance Capacity After Aerobic Training in Previously Untrained Women. Am. J. Clin. Nutr. 2004, 79, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Brutsaert, T.D.; Hernandez-Cordero, S.; Rivera, J.; Viola, T.; Hughes, G.; Haas, J.D. Iron Supplementation Improves Progressive Fatigue Resistance during Dynamic Knee Extensor Exercise in Iron-Depleted, Nonanemic Women. Am. J. Clin. Nutr. 2003, 77, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Goodman, C.; Peeling, P.; Ranchordas, M.K.; Burke, L.M.; Stear, S.J.; Castell, L.M. A to Z of Nutritional Supplements: Dietary Supplements, Sports Nutrition Foods and Ergogenic Aids for Health and performance—Part 21. Br. J. Sports Med. 2011, 45, 677–679. [Google Scholar] [CrossRef] [PubMed]
- Pasricha, S.R.; Low, M.; Thompson, J.; Farrell, A.; De-Regil, L.M. Iron Supplementation Benefits Physical Performance in Women of Reproductive Age: A Systematic Review and Meta-Analysis. J. Nutr. 2014. [Google Scholar] [CrossRef] [PubMed]
- Mielgo-Ayuso, J.; Zourdos, M.C.; Calleja-González, J.; Urdampilleta, A.; Ostojic, S. Iron Supplementation Prevents a Decline in Iron Stores and Enhances Strength Performance in Elite Female Volleyball Players during the Competitive Season. Appl. Physiol. Nutr. Metab. 2015, 40, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, Y.O.; Schmid, A.; Grathwohl, D.; Bultermann, D.; Berg, A. Hematological Indices and Iron Status in Athletes of various Sports and Performances. Med. Sci. Sports Exerc. 2002, 34, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Zourdos, M.C.; Sanchez-Gonzalez, M.A.; Mahoney, S.E. A Brief Review: The Implications of Iron Supplementation for Marathon Runners on Health and Performance. J. Strength Cond. Res. 2015, 29, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, P.; Nachtigall, D. Iron Supplementation in Athletes: Current Recommendations. Sports Med. 1998, 26, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J.; Shirreffs, S.M. Nutrition and Hydration Concerns of the Female Football Player. Br. J. Sports Med. 2007, 41 (Suppl. 1). [Google Scholar] [CrossRef] [PubMed]
- Newhouse, I.J.; Clement, D.B.; Taunton, J.E.; McKenzie, D.C. The Effects of Prelatent/Latent Iron Deficiency on Physical Work Capacity. Med. Sci. Sports Exerc. 1989, 21, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and Athletic Performance. J. Acad. Nutr. Diet. 2016, 116, 501–528. [Google Scholar] [CrossRef] [PubMed]
- Otten, J.J.; Hellwig, J.P.; Meyers, L.D. Institute of Medicine. Dietary Reference Intakes: The Essential Guide to Nutrient Requeriments; The National Academies Press: Washington, DC, USA, 2006; p. 543. [Google Scholar]
- Abbaspour, N.; Hurrell, R.; Kelishadi, R. Review on Iron and its Importance for Human Health. J. Res. Med. Sci. 2014, 19, 164–174. [Google Scholar] [PubMed]
- Kim, I.; Yetley, E.A.; Calvo, M.S. Variations in Iron-Status Measures during the Menstrual Cycle. Am. J. Clin. Nutr. 1993, 58, 705–709. [Google Scholar] [CrossRef] [PubMed]
- Reinke, S.; Taylor, W.R.; Duda, G.N.; von Haehling, S.; Reinke, P.; Volk, H.D.; Anker, S.D.; Doehner, W. Absolute and Functional Iron Deficiency in Professional Athletes during Training and Recovery. Int. J. Cardiol. 2012, 156, 186–191. [Google Scholar] [CrossRef] [PubMed]
- DellaValle, D.M. Iron Supplementation for Female Athletes: Effects on Iron Status and Performance Outcomes. Curr. Sports Med. Rep. 2013, 12, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Thomas, L. Clinical Laboratory Diagnostics: Use and Assessment of Clinical Laboratory Result, 1st ed.; TH Books: Frankfurt, Germany, 1998; p. 1527. [Google Scholar]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and Validation of a Food Frequency Questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Mielgo-Ayuso, J.; Collado, P.S.; Urdampilleta, A.; Martínez-Sanz, J.M.; Seco, J. Changes Induced by Diet and Nutritional Intake in the Lipid Profile of Female Professional Volleyball Players After 11 Weeks of Training. J. Int. Soc. Sports Nutr. 2013, 10, 55. [Google Scholar] [CrossRef] [PubMed]
- Farrán, A.; Zamora, R.; Cervera, P. Tablas de Composición de Alimentos del Centre D’Ensenyament Superior de Nutrició i Dietètica (CESNID); Universitat de Barcelona: Barcelona, Spain, 2004. [Google Scholar]
- Peeling, P.; Sim, M.; Badenhorst, C.E.; Dawson, B.; Govus, A.D.; Abbiss, C.R.; Swinkels, D.W.; Trinder, D. Iron Status and the Acute Post-Exercise Hepcidin Response in Athletes. PLoS ONE 2014, 9, e93002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auersperger, I.; Knap, B.; Jerin, A.; Blagus, R.; Lainscak, M.; Skitek, M.; Skof, B. The Effects of 8 Weeks of Endurance Running on Hepcidin Concentrations, Inflammatory Parameters, and Iron Status in Female Runners. Int. J. Sport Nutr. Exerc. Metab. 2012, 22, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, K. Numerical Methods for Estimating Iron Requirements from Population Data. Biol. Trace Elem. Res. 2003, 95, 155–172. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Adecuate Iron Stores | Funtional Iron Deficency | Absolute Iron Deficency | Anemia | p | |
|---|---|---|---|---|---|
| CG | |||||
| T11 | 0 (0) | 7 (63.6) | 4 (36.4) | 0 (0) | 0.157 |
| T29 | 1 (9.1) | 7 (63.6) | 3 (27.3) | 0 (0) | |
| ITG | |||||
| T11 | 2 (18.2) | 7 (63.6) | 2 (18.2) | 0 (0) | 0.046 |
| T29 | 1 (9.1) | 6 (54.5) | 4 (36.4) | 0 (0) | |
| Unstandardized Coefficients | Standardized Coefficients | t | Sig. | R2 Adjust | ||
|---|---|---|---|---|---|---|
| B | Std. Error | Beta | ||||
| ∆ Half-squat | ||||||
| (Constant) | −8.588 | 3.361 | −2.555 | 0.031 | ||
| ∆TRF | −0.967 | 0.332 | −0.696 | −2.910 | 0.017 | 0.427 |
| ∆ Pull Over | ||||||
| (Constant) | 3.539 | 2.470 | 1.433 | 0.186 | ||
| ∆FER | 0.123 | 0.032 | 0.788 | 3.839 | 0.004 | 0.580 |
| ∆ Total Mean Strength | ||||||
| (Constant) | −2.735 | 1.481 | −1.847 | 0.098 | ||
| ∆TRF | −0.501 | 0.148 | −0.578 | −3.387 | 0.008 | 0.689 |
| ∆FER | 0.048 | 0.015 | 0.556 | 3.259 | 0.010 | |
| CON | ITG | p | RDA * | |
|---|---|---|---|---|
| Energy (kcal) | 2744.5 ± 21.6 | 2792.4 ± 34.4 | 0.279 | |
| Total Carbohydrates (g) | 288.6 ± 24.2 | 306.22 ± 22.0 | 0.105 | |
| Total Proteins (g) | 134.6 ± 14.2 | 138.2 ± 19.3 | 0.648 | |
| Animal Proteins (g) | 91.16 ± 15.6 | 95.2 ± 19.0 | 0.618 | |
| Vegetable Proteins (g) | 43.6 ± 6.1 | 43.2 ± 3.5 | 0.856 | |
| Total Fats (g) | 111.4 ± 9.0 | 108.7 ± 8.8 | 0.515 | |
| Ca (mg) | 1168.5 ± 60.2 | 1166.7 ± 66.8 | 0.984 | 1000 |
| Mg (mg) | 541.0 ± 31.3 | 554.5 ± 17.9 | 0.699 | 310 |
| P (mg) | 2106.1 ± 45.0 | 2126.2 ± 84.4 | 0.846 | 700 |
| Fe (mg) | 22.1 ± 1.5 | 23.52 ± 1.12 | 0.454 | 18 |
| Zn (mg) | 14.0 ± 0.3 | 14.4 ± 0.7 | 0.605 | 8 |
| Vitamin A (µg) | 1791.3 ± 300.3 | 1862.9 ± 247.5 | 0.708 | 700 |
| Vitamin E (mg) | 18.3 ± 1.2 | 15.5 ± 0.7 | 0.051 | 15 |
| Thiamine (mg) | 2.52 ± 0.08 | 2.43 ± 0.14 | 0.604 | 1.1 |
| Riboflavin (mg) | 2.70 ± 0.06 | 2.79 ± 0.17 | 0.678 | 1.1 |
| Niacin (mg) | 37.9 ± 2.2 | 38.9 ± 2.3 | 0.749 | 14 |
| Vitamin B6 (mg) | 3.77 ± 0.19 | 3.82 ± 0.25 | 0.868 | 1.3 |
| Folic Acid (µg) | 624.8 ± 47.7 | 621.3 ± 39.9 | 0.955 | 400 |
| Vitamin B12 (µg) | 9.24 ± 0.99 | 9.96 ± 2.01 | 0.767 | 2.4 |
| Vitamin C (mg) | 358.4 ± 47.7 | 371.4 ± 36.6 | 0.829 | 75 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mielgo-Ayuso, J.; Zourdos, M.C.; Calleja-González, J.; Córdova, A.; Fernandez-Lázaro, D.; Caballero-García, A. Eleven Weeks of Iron Supplementation Does Not Maintain Iron Status for an Entire Competitive Season in Elite Female Volleyball Players: A Follow-Up Study. Nutrients 2018, 10, 1526. https://doi.org/10.3390/nu10101526
Mielgo-Ayuso J, Zourdos MC, Calleja-González J, Córdova A, Fernandez-Lázaro D, Caballero-García A. Eleven Weeks of Iron Supplementation Does Not Maintain Iron Status for an Entire Competitive Season in Elite Female Volleyball Players: A Follow-Up Study. Nutrients. 2018; 10(10):1526. https://doi.org/10.3390/nu10101526
Chicago/Turabian StyleMielgo-Ayuso, Juan, Michael C. Zourdos, Julio Calleja-González, Alfredo Córdova, Diego Fernandez-Lázaro, and Alberto Caballero-García. 2018. "Eleven Weeks of Iron Supplementation Does Not Maintain Iron Status for an Entire Competitive Season in Elite Female Volleyball Players: A Follow-Up Study" Nutrients 10, no. 10: 1526. https://doi.org/10.3390/nu10101526