
UVic Professor Kelli Stajduhar, left, and Paige Phillips are photographed during the National Day of Action on the Overdose Crisis outside of the Ministry of Health building in Victoria, B.C.Chad Hipolito/The Globe and Mail
“Feeling optimistic,” Grant Schlotter wrote on Facebook on Aug. 14, 2018.
In the post, he announced to family and friends that he was in a Victoria hospital, where he was being nursed back to health. Mr. Schlotter – Myster to his friends – was a hockey fan, a cat lover, a one-time insurance broker and a drug user.
In Victoria’s street community, he was a highly-regarded harm-reduction advocate.
But days after Mr. Schlotter’s post, the 55-year-old was on life support with no chance of recovery, resulting from complications from his hard-lived life.
What happened next is helping change the way high-risk populations face death.
Thousands of Canadians are dying each year because of the opioid crisis. Few have planned for a death with dignity. But Mr. Schlotter did. He made sure the people he regarded as his street family knew what he wanted, right down to the songs he would like played at his funeral. The playlist was honoured, but in most other respects, his friends were powerless to ensure he died as he wished.
Now, a group of front-line workers and palliative-care experts have joined forces in Victoria to help those most at risk of an untimely death to make effective end-of-life plans. They are adapting the principles of palliative care – from pain management to emotional support for those who are dying – to the needs of vulnerable and marginalized populations.
Mr. Schlotter knew the risks he faced because of his drug use. He wrote a will shortly before his death. His few possessions, including his treasured Detroit Red Wings hockey jersey, were to be distributed to the people he considered his street family.
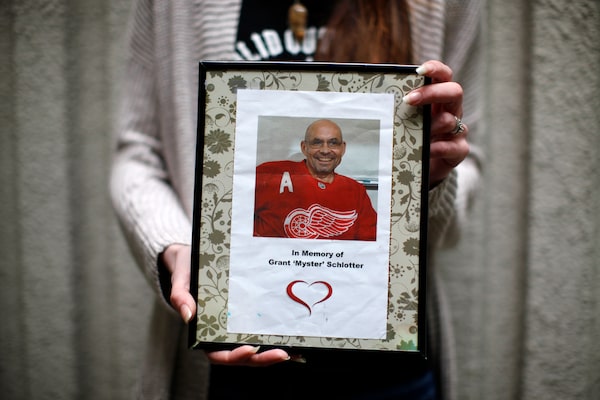
Paige Phillips holds a picture of her friend Grant 'Myster' Schlotter during the National Day of Action on the Overdose Crisis outside of the Ministry of Health building in Victoria, B.C., April 16.Chad Hipolito/The Globe and Mail
But his street family could not direct medical staff about his treatment. His possessions were tossed in the garbage at the single-room occupancy hotel where he was living.
“It was the worst,” said Paige Phillips, the peer-support worker who had signed his will as a witness. She got the crumpled document back only because a neighbour retrieved it from the trash. “It felt really hopeless – sickening – that I couldn’t deliver it for him.”
Since Mr. Schlotter’s death, Ms. Phillips has relived the trauma of sitting with a dying friend again and again, each time trying to advocate for them but often being dismissed. She has used those deaths to shape a plan to help members of her community make an advanced care plan, so they can die on their own terms.
Kelli Stajduhar, a professor of nursing with the University of Victoria’s Institute on Aging, is leading the project. Prof. Stajduhar has worked in palliative care for three decades and her research has exposed how poorly the most vulnerable populations are served at the end of their lives.
Few Canadians have good end-of-life planning in place, she said, but usually family members can help advocate for their loved ones. However, being part of a tight-knit street family carries no legal weight.
“They are not typically listened to by the health-care system,” Prof. Stajduhar said. “So, people are screwed.”
The project has two parts.
One is reaching out to Victoria’s street community population, getting people to sit down and make an advanced care plan for their death and to answer questions such as: If you are nearing death, who can speak for you? Do you want to be at home, on the street or in a hospital? At what point do you want to stop life-prolonging medical interventions?
The other is ensuring those plans are recognized by those who deliver end-of-life care. Prof. Stajduhar’s team is engaging health-care workers in acute-care settings, as well as those who run supportive housing and shelter workers.
The group is testing and piloting the tools as they go. Prof. Stajduhar has tapped into the “lived experience” of community workers such as Ms. Phillips, who provide a bridge between university researchers, service providers and the street populations they want to reach.
Ashley Mollison, the project co-ordinator, said advanced care planning is not just about death.
“This is about people having a greater say in their health care during their life. You never know what’s going to happen, especially in the context of the overdose crisis,” she said. “This can be for anybody. I mean, I should do it. It’s for everybody.”
Another member of the project is Kimmie Hughes, a Métis woman who grew up on the streets, where she is known as Mama. She is a health-education co-ordinator at Solid Outreach, an organization of current or former illicit-drug users in Victoria.
“I’ve seen a lot of deaths, especially lately with the overdose crisis. A lot of people have died all alone, in a hospital. It’s really hurtful," she said. Helping people understand that they can shape the circumstances of their death, she said, is a powerful change. “When you have more say, you are not too afraid.”
Heather Hobbs, the manager for harm reduction at AIDS Vancouver Island, attended Mr. Schlotter’s funeral, which drew a huge crowd. She remembered him as “a lovely human being” and a tireless advocate for the city’s most marginalized residents. He wanted to break down stigmas about drug users.
“He was a dude who lived a heavy life, who helped others,” she said. “It’s tragic that he didn’t get the end he wanted.”
Less than a year before his death, Mr. Schlotter published an essay in which he described his years spent in shelters, detox facilities and recovery houses. He had periods of homelessness. He did jail time. He tried and failed to beat his addictions.
“My only real expertise seems to lie in my lifelong use of mind-altering substances and dealing with the often harmful consequences of their use,” he wrote.
In the end, he found peace working as a peer navigator, helping others in his community connect with detox services and housing. “The past couple of years have been very exciting and productive for me as a I found a place where I have been accepted and even appreciated for just being me.”
Last December, Ms. Phillips found herself once again at the side of a friend. Douglas Oliver, 62, was considered an elder of the community. Along with Mr. Schlotter, they helped change the way the public sees the opioid crisis when he convinced health authorities to change an ad campaign warning about the dangers of fentanyl in street drugs. Instead of a stark image of a toe tag on a cadaver, the ads now focus on the fact that those at risk are real people.
Mr. Oliver was working at Victoria’s supervised drug-use site when he had a stroke.
“He revived countless individuals and responded to some of the most complicated overdoses,” she recalled. “I don’t know how many people – mothers, daughters, sisters and friends – still have their lives today because of him.”
But his own drug use took a toll on his health. Recently, he was dying in an emergency room where clinical staff couldn’t provide the death he had wanted.

There are roughly 10 Canadians dying from drug overdoses every day.Chad Hipolito/The Globe and Mail
She knew he wanted a controlled MAiD death – Canada’s medical assistance in dying option. But the ER doctors were unconvinced and instead withdrew his life-preserving antibiotics.
“We knew exactly what he did want and what he didn’t want. ... We had it all documented. But because there was a communication gap, we didn’t get there. He died a natural death, alone. And his family wasn’t prepared for it. It was traumatic.”
There are roughly 10 Canadians dying from drug overdoses every day. Death, for street-community populations, is now a numbingly common event. But by learning from how Mr. Oliver and Mr. Schlotter died, Ms. Phillips said she can see, already, that the project is making a difference.
In January, she was asked to meet a dying woman, named Jess, who had acute endocarditis – an infection in the blood that can settle in the heart. Intravenous drug users are at high risk and along with the spike in OD deaths, these infections are increasingly common.
This was Jess’s fourth bout of endocarditis and this time doctors found clots in her brain and her lungs. One or the other was going to kill her, the doctors explained.
“Her family didn’t want to make the decision,” Ms. Phillips said.
For the third time in months, she was delegated to make life and death decisions. She celebrated Jess’s 31st birthday with her, in hospital, as they planned what to do.
“We made the decision together, with her birthday cake.” This time, Jess’s voice was heard.
 Justine Hunter
Justine Hunter